We all know that a comfortable pair of shoes can make a day on your feet much more enjoyable. But what is a “comfortable shoe?” In today’s market there are countless options for shoe types, styles, support levels, etc. Here are a few basic guidelines to help you pick a shoe that will allow you to go the extra mile.
Bend and Twist
The first thing you should do when shoe shopping is pick up the shoe and start bending and twisting it. If you are looking for more support, the shoe should only bend in the toes, not in the arch. A stiffer shoe can help with heel pain, arch pain, and pain in the ball of the foot.
Toe Box – Upper Material
A “natural toe box” can allow more room for your toes to move freely. A natural toe box will be wider and deeper than a traditional shoe. These are usually best for people with toe deformities like bunions and hammertoes as they provide more room for the toes to move.
If you do have toe deformities, then an upper material that is soft and pliable will decrease pressure, prevent calluses, and reduce pain. Stay away from shoes with stiffer leather or those that have stitching/designs over the toes.
Length & Width
Shoes should be one thumb-width longer than your longest toe when you are standing. Remember, if you wear a size 8 in one shoe brand, that doesn’t mean you will wear a size 8 in all shoe brands.
If shoes feel too tight or constricting while trying them on, do not think “they will stretch.” Get a larger size. Your feet swell as the day goes on, so it is best to go shoe shopping in the afternoon. If you wear orthotics be sure to bring those with when you are shopping for shoes.
Cushioning
While a thicker sole can feel better on arthritic feet, it is more important that the sole does not bend in the arch. Find a stiff shoe first and then find one with your ideal amount of cushion.
Beware of shoes with too much cushion because they can make you feel unstable, and you could twist your ankle.
Rocker Bottom Sole
Athletic shoes offer a rocker bottom which can be helpful for people with pain in the ball of their feet or in their Achilles tendon. However, they can also cause overloading of the knee joint and knee pain. If you do buy these shoes because you have forefoot pain, be sure to wear them only occasionally.
Zero Drop Shoes
In most shoes, even those without a noticeable “heel,” the heel sits higher than the toe of the shoe. Zero drop shoes have no difference between the heel and the toe. This mimics a “barefoot” style of walking which can lead to increased stretching of the Achilles tendon and strengthening of the calf muscles. It can also relieve pressure on the ball of your foot. But these shoes can also lead to overuse injuries of the Achilles tendon so you should gradually transition to wearing them and avoid frequent use.
Tread
Tread helps your shoes grip different surfaces, so it is important to choose the right shoe for certain activities. You should not wear gym shoes when hiking and you should not wear trail shoes for playing basketball. Just because a shoe is comfortable playing pickleball doesn’t mean it will be comfortable hiking the Grand Canyon.
Quality Over Style
It is more important to choose a shoe that is better quality than the style or color that you want. This is especially true if it is a shoe that you will be doing a lot of activity in. One theory is “the more you behave, the more you can cheat.” In other words, if you want to wear stylish shoes to dinner on Saturday night, you better wear good supportive shoes during the day.
It can be easy to get overwhelmed when you are trying to pick out the perfect pair of shoes. Remember that these are all guidelines and not hard rules. If the shoe feels comfortable to you and doesn’t cause any pain, go ahead and wear it. If no shoes seem to help with your foot issues, it may be time for a visit with a podiatrist.
Podiatrist, Dr. David Arens, sees patients at Lakeview Clinic in Waconia and Chaska, MN. His practice involves all aspects of podiatric medicine and surgery. He performs surgery of all foot and ankle conditions ranging from bunions and hammertoes to fractures and chronic ankle pain. He believes in the importance of listening to the patient to develop the best specific treatment plan for each individual.
Lakeview providers address common colonoscopy concerns, fears, and questions.
It is estimated that about 1 in 24 people will develop colorectal cancer at some point in their lifetime, and colonoscopies are the best preventative measure currently available. “The only people dying from colon cancer, are the people who are not getting a colonoscopy” states Lakeview Physician, Dr. Paul Brown. Despite this, many people choose not to follow the advice of their medical provider when they are told to have a colonoscopy screening.
There are a variety of reasons people avoid or delay getting colonoscopies, even though they are an important tool for detecting colorectal cancer and other gastrointestinal issues. A panel of Lakeview Clinic medical providers has addressed many of these reasons below in an effort to persuade patients to have this important screening and potentially save lives.
I have no family history of colon cancer; is a screening necessary?
“Current recommendations for colonoscopy in patients without family history begins at age 45,” states Dr. Todd Elftmann. Colorectal cancer can develop without noticeable symptoms, and early detection is crucial. According to Dr. Timothy Thormodsgard, “The majority of colon cancer cases occur in people with no family history of colon cancer, so screening is important even if you have no family history.”
Isn’t it possible that polyps aren’t cancerous?
Knowing whether a polyp in benign (non-cancerous) is critical to preventing colon cancer. “The only way to know which type of polyp you may have is to do a colonoscopy. Additionally, the polyp can usually be removed during the procedure, which will prevent it from becoming a cancer” states Dr. Thormodsgard.
“Not all polyps are harmful but monitoring them closely can help prevent colon cancer and save your life” explains Dr. Heidi Wuerger. If no polyps are found, the study should be repeated in 10 years.
What if polyps are found?
Dr. Elftmann explains, “we do not always know which polyps we encounter will actually become cancer. Therefore, [polyps] will be removed and sent to a pathologist. The pathologist will determine if the polyp is pre-cancerous, and recommendations regarding appropriate follow-up will be made.” If adenomatous polyps are found, the study will likely need to be repeated in 3-5 years depending on the number and type of polyps found.
I’ve heard polyps can be missed. If so, why even get a colonoscopy?
Dr Thormodsgard explains, “there is a risk that a polyp will not be seen during the colonoscopy. Research has shown that nearly 17% of polyps can be missed during the exam. However, that means that over 80% of polyps are found and treated during the exam. The polyps that are missed are almost all less than 1 centimeter in size. Additionally, the risk of missing colon cancer during a colonoscopy is very low, around 2-3%. Because we know that some polyps are at risk of developing into colon cancers, and that this transformation happens slowly, getting a colonoscopy is still the best way to prevent colon cancer.
I am nervous about complications.
Dr. Todd Elftman outlined complication rates as follows: “Complications include bleeding are 8 in 10,000; colon perforations are 4 in 10,000, and the risk of death is 3 in 100,000.” In comparison, “the risk of death in a car accident is approximately 1 in 100.” In addition to complications being very rare, they are also treatable. According to Dr. Heidi Wuerger, “if a perforation and bleeding do happen, there are good means to help treat these complications.” It also bears mentioning that, according to The American Cancer Society, the rate of developing colon/rectum cancer is 1 in 24 for males and 1 in 26 for females.
I’m terrified of anesthesia. What can alleviate this concern?
Colonoscopies take about 20 minutes and are typically done with conscious sedation “In general, the anesthesia used for a colonoscopy is very safe. Your vital signs will be closely monitored throughout the procedure” stated Dr. Thormodsgard. Dr. Wuerger added that patients “could do a small pre-medication, if needed.”
Do colonoscopies hurt?
According to Dr. Brown, “people may have mild discomfort during the procedure and for a day or so afterwards.” “Patients usually will not remember any discomfort during the procedure due to the sedative medications,” adds Dr. Elftmann.
How bad is preparation for a colonoscopy?
“The colonoscopy preparation is usually the worst part for about 95% of patients. However, if the preparation is taken as instructed, most patients tolerate the preparation quite well and without issues. Some patients experience nausea and vomiting, but this is usually due to patients trying to rush the oral intake rather than following the timing of oral intake in the directions they receive. I recommend giving yourself plenty of time the evening before and the morning of the colonoscopy to complete the preparation,” explains Dr. Elftmann.
If I am diabetic, will preparing for a colonoscopy be hard on me?
Be sure to talk with your primary medical provider about any concerns. They are your go-to for advice regarding safely preparing for a colonoscopy. Whether it is adjusting medications or recommending different insulin doses, they are best equipped to assist you. Additionally, “you are able to consume a clear liquid diet before, during, and after your bowel preparation. This will allow you to maintain your glucose intake and levels,” adds Dr. Elftmann.
How much time will I need to take off of work?
Typically, one day is needed. “You will need to begin your bowel preparation in the early evening the day before your colonoscopy and will need to take the day off for your colonoscopy. Most people are back to normal activities without restrictions the day following their procedure,” explains Dr. Elftman.
Why not just do a Cologuard test instead?
Put simply, “it is less sensitive and if positive, you will require a colonoscopy anyway,” states Dr. Brown. “Unfortunately, there are numerous limitations to the Cologuard test. The test can miss up to 8% of colon cancers and 42% of polyps, giving a false negative result,” adds Dr. Thormodsgard. Dr. Elftmann says another way to look at it is “Cologuard will not detect a colon cancer when present approximately 8% of the time and will not detect an advanced pre-cancerous polyp when present approximately 58% of the time.” When early detection is so important in saving lives, these numbers really matter.
Some patients may have health or medical statuses that prevent them from undergoing a colonoscopy. Cologuard is an option for these patients.
Does insurance cover colonoscopies?
We always recommend verifying coverage with your insurance company prior to having any procedure, but in general, colonoscopy screenings are considered preventative and therefore covered. However, if the patient has any gastrointestinal symptoms, or your doctor finds a polyp or mass needing biopsy, your colonoscopy is then considered diagnostic, and your coverage may change. Patients may be required to pay a deductible or coinsurance for a diagnostic colonoscopy.
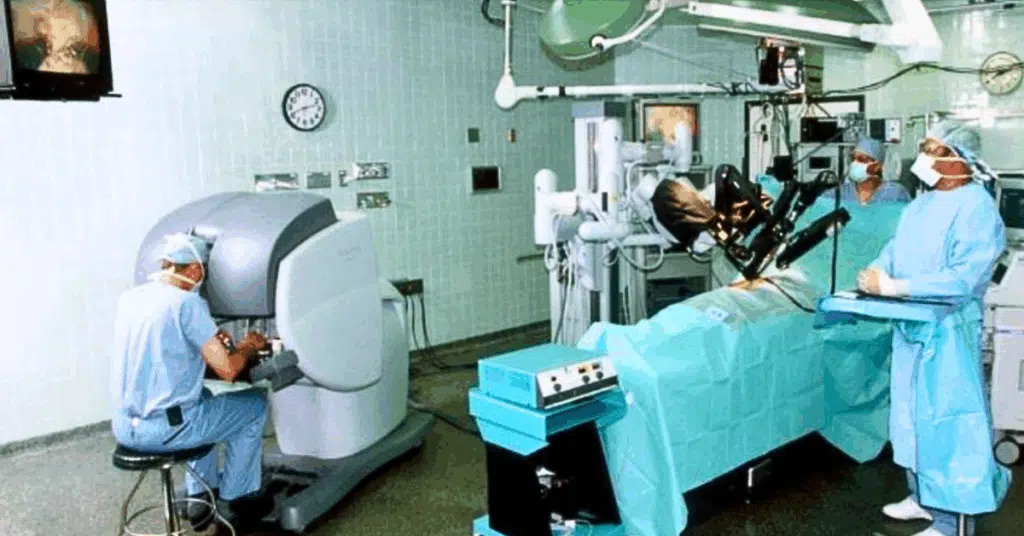
In medicine, something we can all expect is change. Surgical care is no different than other specialties and the most recent significant change within the surgical community is the utilization of robotics. At Lakeview Clinic, we have several of our surgeons who are trained robotically and have been community leaders in the advancement of robotic surgery using the daVinci Surgical System.
Advantages of Robotic Surgery
Robotic surgical procedures are minimally invasive procedures that have resulted from the advancement of well accepted laparoscopic procedures. The major advantage of using robotics rather than standard laparoscopic procedures is the ability of robotic techniques to simplify fine movements and stabilize the surgeon’s implementation of certain maneuvers. This results in the simplification of standard laparoscopic procedures and improving techniques allowing completion of more complex surgical procedures, previously requiring larger “open” surgical incisions.
How Robotics are Used During Surgery
Robotic surgical procedures still require significant surgeon involvement, as all the technical aspects of the procedure involve human input. This begins with the placement of abdominal cannulas (tubes) which are used to introduce instruments into the abdomen. There will be 3 or 4 cannulas placed through incisions as small as 8 millimeters (about 1/3 of an inch). Through the cannulas, a high-definition video camera and robotic instruments are placed into the abdomen, and the robot is docked to the cannulas. Once the robot is docked, the surgeon sits at the console within the operating room and views images from the high-definition video camera. Using a combination of hand and foot controls, the significant components of the surgical procedure are completed using the robot.
Who Performs Robotic Assisted Surgery?
At Lakeview Clinic, both our general surgeons and gynecologic surgeons perform robotic surgical procedures routinely. The most common procedures include abdominal wall hernia repair, gallbladder removal, hiatal hernia repair, hysterectomy, intestinal resections (particularly colon resections), and ovary and fallopian tube procedures. Many other less common procedures may also be performed using the robotic platform.
The Benefits
The minimally invasive techniques of robotic surgery result in decreased postoperative pain, shorter recovery times, reduced blood loss, shorter hospital stays, shorter operative times and a decrease in certain short-term and long-term postoperative complications. You can read or view a patient’s first-hand account on Ridgeview Foundation’s website. In Russ’s Story he talks about how well he felt post-surgery.
It is important to remember that not all surgical procedures are best performed using robotic techniques for a variety of reasons. Your surgeon can discuss whether a robotic approach is appropriate for you.
Dr. Elftmann joined Lakeview Clinic as a general surgeon in 1995. He has received additional training for complex robotic surgical cases including colon, gastric, as well as hiatal and abdominal wall hernia procedures. Dr. Elftmann has also been recognized as a Minnesota Monthly Top Doctor of General Surgery
It is important to acknowledge that prenatal care is done on an individual basis and can vary significantly depending on maternal and/or fetal conditions. The following outlines a typical schedule of obstetric visits and what you can expect during prenatal care. The Lakeview Clinic OB/GYN team takes pride in providing outstanding, evidence-based care to each of our patients.
Lakeview Clinic’s OB/GYN providers deliver compassionate, high-quality care for expecting mothers.
First Trimester Visits
5-7 Weeks Gestation
At this visit, we will confirm pregnancy, discuss personal medical risks and medication safety. Due dates will be calculated as well and are typically based on first day of last menstrual period. Other topics may include early pregnancy symptoms and concerning signs/symptoms of potential issues such as miscarriage and ectopic pregnancy.
8-9 Weeks Gestation
At this point, an optional early pregnancy ultrasound can be performed by one of the OB/GYN physicians in the office. This allows for confirming and establishing the due date, the viability, and number of fetuses.
11-13 Weeks Gestation
This is the first OB visit where your medical history is reviewed, blood work is done including optional noninvasive prenatal testing (NIPT), and we listen to the fetal heartbeat.
Second Trimester Visits
Prenatal visits typically occur every 4 weeks (16, 20, 24, and 28 weeks) with an OB physician.
20 Weeks Gestation
A fetal anatomy survey is performed in order to evaluate the fetal, maternal, and placental anatomy and confirm the estimated due date/size of the baby. This can be done in our clinic by an ultrasound technologist. The ultrasound is then read by a radiologist who will review the survey with your OB physician
26-28 Weeks Gestation
Blood work is done to evaluate for gestational diabetes, anemia, etc., Tdap vaccine and Rhogam if needed are also recommended.
Third Trimester Visits
30 Weeks Gestation
At this point prenatal visits become more frequent and take place every 2 weeks. These more frequent visits are recommended to closely monitor blood pressure and fetal growth.
36 Weeks Gestation
During this visit, a Group B Strep test is performed, and fetal presentation is confirmed (We are looking to see that baby is head down; we use the term Vertex presentation). We can tell this either by cervical check or a brief ultrasound that the OB does to confirm. Weekly visits start now.
When it is Time for Baby’s Arrival
All of our patients deliver at Ridgeview’s Birthing Center. The birthing center has six private labor rooms. Two of the rooms have large tubs and all have showers.
While we all thoroughly enjoy attending the deliveries of our own patients this is not always possible. In general, we try our best to be there for our patient’s labor and delivery. If we are unavailable, one of the other Lakeview OB partners who is on call will attend and take great care of you during labor and delivery. You can also expect to see one of us every day that you are in the hospital both while in labor and postpartum. We are also happy to help you get established with an experienced provider for newborn care at Lakeview Clinic. Newborn visits are available daily. We also follow up with you in the office 6 weeks postpartum and sooner whenever needed. Our patients are our priority, and we welcome and accept newly pregnant patients every day.
Dr. Erin Chinnock sees patients at Lakeview in Chaska and Waconia. Her practice involves both obstetrics and gynecology. She cares for patients with a wide variety of concerns related to reproductive health, pregnancy, and menopause. Her areas of interest include preventative care, low and high-risk obstetrics, contraception and sexual health.
Dr. Heidi Wuerger’s Experiences Through Volunteering
Sometimes when I’m not in the office, Watertown staff ask “where’s Dr. Wuerger? Much of that time has been spent volunteering in places as far as Ecuador. In the last year I have been fortunate enough to spend time on 3 service trips. At Lakeview Clinic, part of our mission is service and Lakeview clinic employees serve every day in and out of the clinic.
In August of 2023, I spent a week in Belize with my church as an adolescent Leader. We had a group of 54 people who spent time in the city of San Antonio on the western side of Belize near Guatemala, and Bermudian Landing near Belize City. We ran children’s camps, dug trenches, helped clean up a recreation camp, delivered food to underserved at their homes and developed international friendships and knowledge. We also learned how difficult it can be to get a high school education, much less a college or medical school education, which only exists in Belize city. This is one of the reasons Belizeans do not have access to occupational or speech therapy and have very little physical therapy.
In January to February this year I spent 2 weeks with Common Ground International in a medical Spanish immersion program in Costa Rica. Rory and Leslie, the co-owners and founders of common ground, have 2 immersion trips -one to Costa Rica and the other to Ecuador. I had made a commitment to learn Spanish, so with the help of Google, I searched Spanish immersion and medical. This led me to Common Ground and in the end of January I found myself flying into San Jose, Costa Rica.
During this trip, I stayed in Santo Domingo de Heredia with a lovely family of 5, including 3 boys ages 5-12. I walked to Spanish school, Lapa Verde each day and spent 4 hours in intense Spanish class every weekday and made the commitment to speak only Spanish for 2 weeks. During this experience, we learned about the culture, donated to the community and helped serve in the community clinics. Multiple days we went to CEDCAS (a non-profit organization in Costa Rica for Health Education and Services) community center and took weight, height, blood pressures, blood sugars, reviewed medications and answered questions. This specific center helps the shanty town area Guarari.
The last week in June I went to Chicago with 26 other adolescents and adults on another service trip. Many kids and families were nervous for the trip due to media reports about Chicago. We stayed in a church and did service events around the city. We learned about refugee resettlement where the main message was that they are people just like us. We bought supplies for 2 different families, one from Bangladesh and the other from Pakistan and then set up their apartments. It was about $750 to set up basic supplies for a family of 4 in one apartment. These families spend on average 5-6 years living in refugee camps with about 14 square foot space and blankets for walls. They go through significant vetting processes to get into the US and have given up their belongings, except if they’re lucky a backpack. Once they arrive, they are required to pay back most of the cost, including their plane tickets
We also worked with A Just Harvest, a greenhouse and garden in the city which serves lunches for the homeless. Another day was spent at Projectcure.org – a medical warehouse where we sorted donated medical supplies to go to countries in need. We also went to Berniesbooks.org -a warehouse filled with new books, where volunteers help organize, label and separate the books that are donated to kids in need in the area.
All of these opportunities allowed people to open their eyes to see people and places differently. It’s amazing to see that process, especially on the face of a teenager. And when people ask ‘Where’s Dr Wuerger’-I might be on another service trip, hopefully meeting more people, learning more Spanish and creating more heartfelt connections in the world. Yet, I know it’s not just happening on these trips but happening in our clinic and our community as well. So, THANK YOU, to all those at Lakeview Clinic and in the surrounding communities who SERVE.
Dr. Heidi Wuerger
Family Physician, Dr. Wuerger has training and experience in the care of patients from infancy through adulthood. She enjoys full spectrum family practice including sports medicine, gynecology procedures and urgent care. When she is not working, Dr. Wuerger enjoys spending time with her family and outdoor pursuits such as camping, gardening and running an apple orchard.